 I have now been on Medicare for 18 months. Fortunately, I have not required significant clinical services and therefore do not have a lot of experience with the financial impact of Medicare. The medical insurance part of Medicare costs between $99.90 per month and $369.10 per month (per person), depending on your income. The poliiticians imply that everybody pays the same for Medicare and it is time for people to pay their fair share. I do not know what would be considered fair, but a range of X to more than 3X is non-trivial. If you want to understand the Medicare premiums in detail, good luck — it is really complicated. Every time I decide to dig into it and understand it, I run out of time and give up. I did have occasion to go to an urgent care center in Florida in January. I contracted a bad case of rhinosinusitis (perhaps from grandchildren, perhaps from inadequate hand washing during the holiday travels) and needed some health care. It took a couple of weeks to get back to normal and then a couple more to get the claims detail from United Health, which is the supplemental medical insurance I get through IBM. It is coordinated with Medicare. In theory, whatever Medicare does not pay goes to the supplemental insurer for consideration. How this works is as clear as mud. Here is what my claim detail from United Health showed for my visit to the doctor at the urgent care center.
I have now been on Medicare for 18 months. Fortunately, I have not required significant clinical services and therefore do not have a lot of experience with the financial impact of Medicare. The medical insurance part of Medicare costs between $99.90 per month and $369.10 per month (per person), depending on your income. The poliiticians imply that everybody pays the same for Medicare and it is time for people to pay their fair share. I do not know what would be considered fair, but a range of X to more than 3X is non-trivial. If you want to understand the Medicare premiums in detail, good luck — it is really complicated. Every time I decide to dig into it and understand it, I run out of time and give up. I did have occasion to go to an urgent care center in Florida in January. I contracted a bad case of rhinosinusitis (perhaps from grandchildren, perhaps from inadequate hand washing during the holiday travels) and needed some health care. It took a couple of weeks to get back to normal and then a couple more to get the claims detail from United Health, which is the supplemental medical insurance I get through IBM. It is coordinated with Medicare. In theory, whatever Medicare does not pay goes to the supplemental insurer for consideration. How this works is as clear as mud. Here is what my claim detail from United Health showed for my visit to the doctor at the urgent care center.
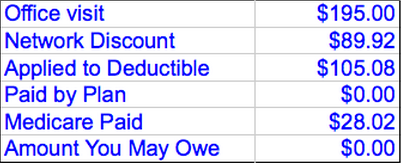
Not to worry. The footnote to the claim detail clears this up (right!).
This Plan Determines Benefits Once Medicare Makes Payment. If Medicare Pays Less Than This Plan’s Benefit, This Plan Will Consider The Difference. This Plan’s Allowable Benefits Are Based On The Medicare Approved Amount If The Physician Or Provider Accepted Medicare’s Assignment Or On The Limiting Charge If They Did Not Accept The Assignment. The Patient Is Responsible For The Difference Between The Allowable Amount And The Total Amount Paid By Both Plans. The Patient Must Pay Any Applicable Plan Deductibles And Copays Before This Plan Can Pay Any Benefits. Medicare payment was applied in the amount of $28.02
There was no co-pay, and if there is a deductible, it would seem that I would have to pay something. What exactly went to whom is a mystery to me. I am sure it is a mystery to our political leaders also. Medicare encourages preventative examinations and tests. That is a good thing, but if I followed all that are recommended, I would be a very busy person. Is there such a thing as too much care? Should care be “rationed”? These terms easily become highly emotional in both clinical and political terms. Some say that Americans have too big of an “appetite” for healthcare services and there is a tug of war going on between the payers, the providers, the patients, and the politicians over what care should be provided. The answer is not more care or less care but more effective care. The entitlement model of paying for more visits, tests, and procedures is what has to change. An emerging new model to address this is called the “Accountable Care Organization” and it will begin the shift from a volume-based system to a value-based system. This is a good thing, and regardless of the 2012 political outomces, I do not see the shift changing.
An ACO relies on close hospital partnerships, collaborative alignment with physicians, robust information technology infrastructure and operational expense management. While the federal government is studying various models, the healthcare industry is moving toward the ACO model which relies on the partnerships between healthcare providers to reduce healthcare costs while maintaining or improving quality of care. Successful ACOs will be rewarded financially, providing additional resources to invest in technology, jobs and other improvements in the delivery of care. The concept of the ACO is to have money flow to the ACO to keep patients healthy and have the money be allocated among the various providers — primary care physicians, specialists, laboratories, imaging centers, etc. Needless to say the method of allocation will make my sinusitis claim detail seem trivial.
One thing is for sure and that is that the current model of care is badly broken and unaffordable. When a 92 year old patient has an indication that a colonoscopy should be performed — knowing that surgery will not be performed regardless of the outcome of the examination — who is benefiting from the expenditure? When an elderly person is incapacitated and a wheelchair can dramatically improve their quality of life then it is a good investment by Medicare. When a person is grossly overweight because they enjoy Krispy Kreme doughnuts, does the spending of millions of dollars on TV advertising to entice that person to get a Medicare-paid “free” sporty electric wheelchair, is that effective or might diet and exercise combined with visits to various members of the ACO be a better investment for Medicare? I think we all know the answer. Be on the lookout for the term ACO. We will be reading much more about this in the local and national news.
